|
|

|

|
| e-Pub |
Section: New Results
New Results
Real-Time Biophysical Models
Deep brain stimulation
Participant : Alexandre Bilger.
During this year, we developed an intra-operative registration method. It is used during a DBS surgery and can help the surgeon to locate anatomical structures for a safer and a more efficient treatment [21] . The method is based on the biomechanical model of brain shift we developed during the last years. Because some parameters of the model are unknown, we propose to estimate them with an optimization process. The cost function evaluates the distance between the model and the segmentation of pneumocephalus, the only indicator of brain shift visible on an intra-operative CT scan.

Stapedectomy
Participant : Guillaume Kazmitcheff.
Stapedectomy is a challenging procedure of the middle ear microsurgery, since the surgeon is in direct contact with sensitive structures such as the ossicular chain. This procedures is taught and performed in the last phase of the surgical apprenticeship. To improve surgical teaching, we propose to use a virtual surgical simulator [26] based on a finite element model of the middle ear. The static and dynamic behavior of the developed finite element model was successfully compared to published data on human temporal bones specimens. A semi- automatic algorithm was developed to perform a quick and accurate registration of our validated mechanical atlas to match the patient dataset. This method avoids a time-consuming work of manual segmentation, parameterization, and evaluation. A registration is obtained in less than 260 seconds with an accuracy close to a manual process and within the imagery resolution. The computation algorithms, allowing carving, deformation of soft and hard tissus, and collision response, are compatible with a real-time interactive simulation of a middle ear procedure. As a future work, we propose to investigate new robotized procedures of the middle ear surgery in order to develop new applications for the RobOtol device and to provide a training tool for the surgeons.
Cardiac electrophysiology
Participant : Hugo Talbot.
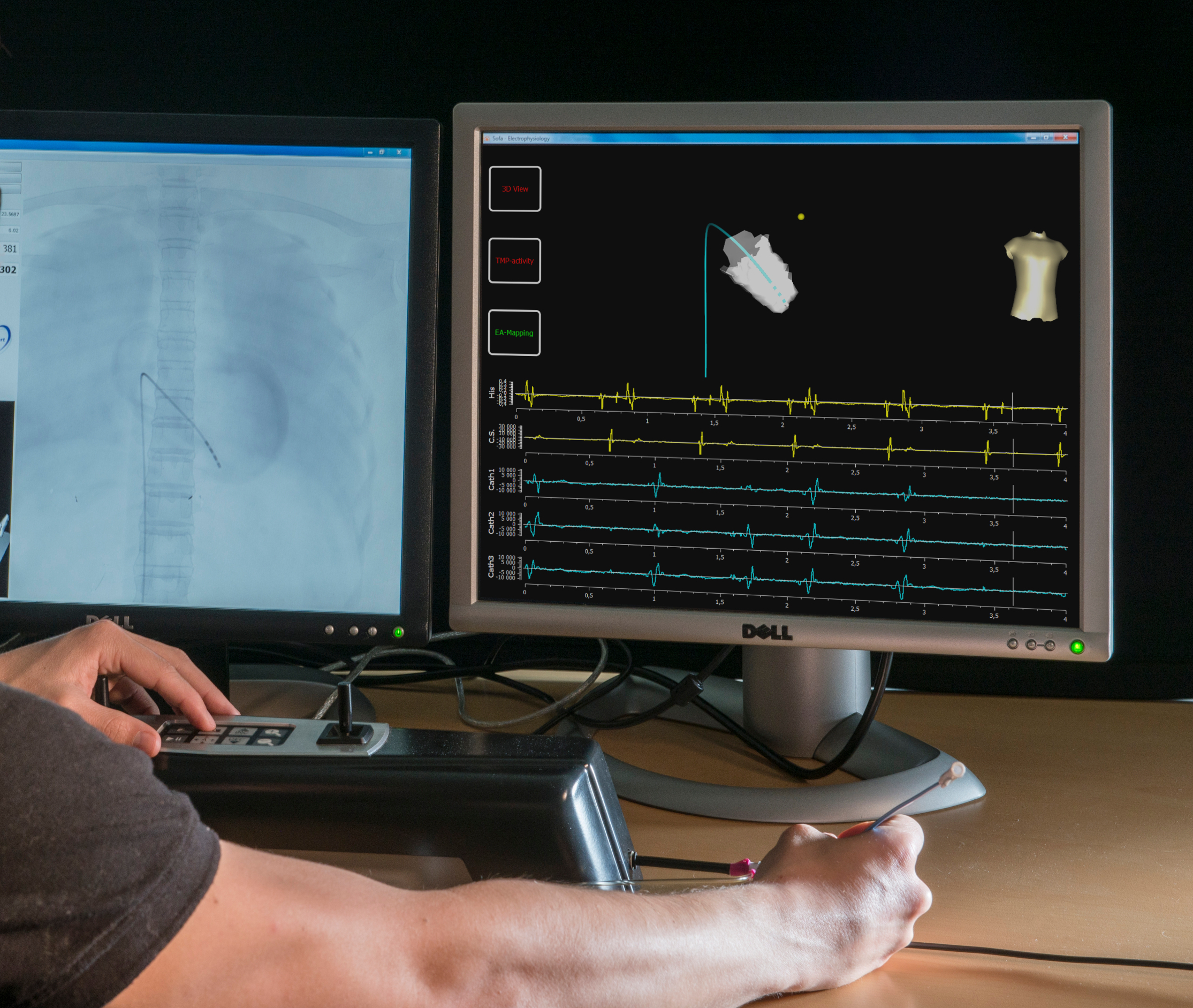
Cardiac arrhythmia is a very frequent pathology that comes from an abnormal electrical activity in the myocardium. The skills required for such interventions are still very challenging to learn, and typically acquired over several years. We first developed a training simulator for interventional electrocardiology and thermo-ablation of these arrhythmias [14] , [32] . Based on physical models, this training system reproduces the different steps of the procedure, including endovascular navigation, electrophysiological mapping, pacing and cardiac ablation. Based on a scenario of cardiac arrhythmia, cardiologists assessed the interactivity and the realism of our simulation.
Beyond electrophysiology training, our work around the cardiac electrophysiology also target the personalization of our mathematical models. Using the dense electrograms recorded intra-operatively, we presented an accurate and innovative approach to personalize our model, i.e. estimate patient-specific parameters. The modeling in silico of a patient electrophysiology is needed to better understand the mechanism of cardiac arrhythmia. This work has been submitted in a conference.
Cryoablation
Participant : Hugo Talbot.
A new project started this year around cryotherapy. This technique consists in inserting needles that freezing the surrounding tissues, thus immediately leading to cellular death of the tissues. Cryoablation procedure is used in many medical fields for tumor ablation, and even starts being used in cardiology. In this scope, we build a simulator able to place the cryoprobes and run a simulation representing the evolution of iceballs in living tissues [31] . This work was presented at MMVR'14.
Connective tissues
Participant : Julien Bosman.
Another topic of simulation is the modeling of connective tissues [18] . First, a comparative study on the influence of the ligaments in liver surgery has been conducted. This study underlines that the model chosen for the ligament's has a strong influence on the outcome of the simulation. More specifically, it shows the the model is at least as much important as the material parameters of the parenchyma. It also shows that the influence of the model depends on the type of effort that is prescribed on the liver. The second axis concerns the validation of a frame (6-DOF nodes) based mechanical model developed for ligaments simulation. Current results show that this model requires less degrees of freedom while providing the same accuracy as a traditional FEM model. At last, a method dedicated to the simulation and the control of continuum robots has been developed. The goal of this method is to replace the mesh of robot by computing its compliance and applying it on a reduced model made of frames. It allows to strongly decrease the number of degrees of freedom needed for the robot simulation while keeping the needed accuracy.
Simulation of lipofilling reconstructive surgery
Participant : Vincent Majorczyk.
We have developed a method to simulate the outcome of reconstructive facial surgery based on fat-filling. Facial anatomy is complex: the fat is constrained between layers of tissues which behave as walls along the face; in addition, connective tissues that are present between these different layers also influence the fat-filling procedure. To simulate the end result, we have proposed a method which couples a 2.5D Eulerian fluid model for the fat and a finite element model for the soft tissues. The two models are coupled using the computation of the mechanical compliance matrix. We had two contributions: a solver for fluids which couples properties of solid tissues and fluid pressure, and an application of this solver to fat-filling surgery procedure simulation.
Inverse FEM simulation
Participant : Eulalie Coevoet.
We introduced a new methodology for semi-automatic deformable registration of anatomical structures [23] , using interactive inverse simulations. We applied the approach for the registration of the parotid glands during the radiotherapy of the head and neck cancer. Radiotherapy treatment induces weight loss that modifies the shape and the positions of these structures and they eventually intersects the target volume. We proposed a method to adapt the planning to limit the radiation of these glands.
|

Numerical Methods for Complex Interactions
Cliping in neurosurgery
Participant : Eulalie Coevoet.
We developed a simulator for neurosurgery. The surgery consist in "clipping" a cerebral aneurysm. Aneurysm is an abnormal local dilatation in the wall of a blood vessel, usually an artery. There are several treatment options for people with the diagnosis of cerebral aneurysm. Medical therapy, surgical therapy (clipping) and endovascular therapy (coiling). The surgical therapy, because of his invasive and technical nature, is the less prescribed. This leads to less and less surgeon trained to practice the procedure. And yet some patients require the surgical way. So the idea was to develop a simulator to train student and also help on the planification.
Virtual cutting
Participants : Huu Phuoc Bui, Christoph Paulus.
The simulation of cutting is a central interest in the team. Several approaches have been investigated this year to model surgical cuts, tearing and other separations of materials induced by surgical tools:
-
using the standard finite element method (FEM) combined with a re-meshing approach, that replaces locally the current structure of the mesh in order to allow for a separation,
-
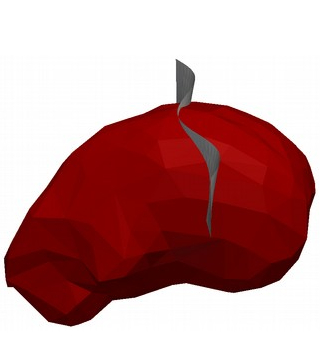
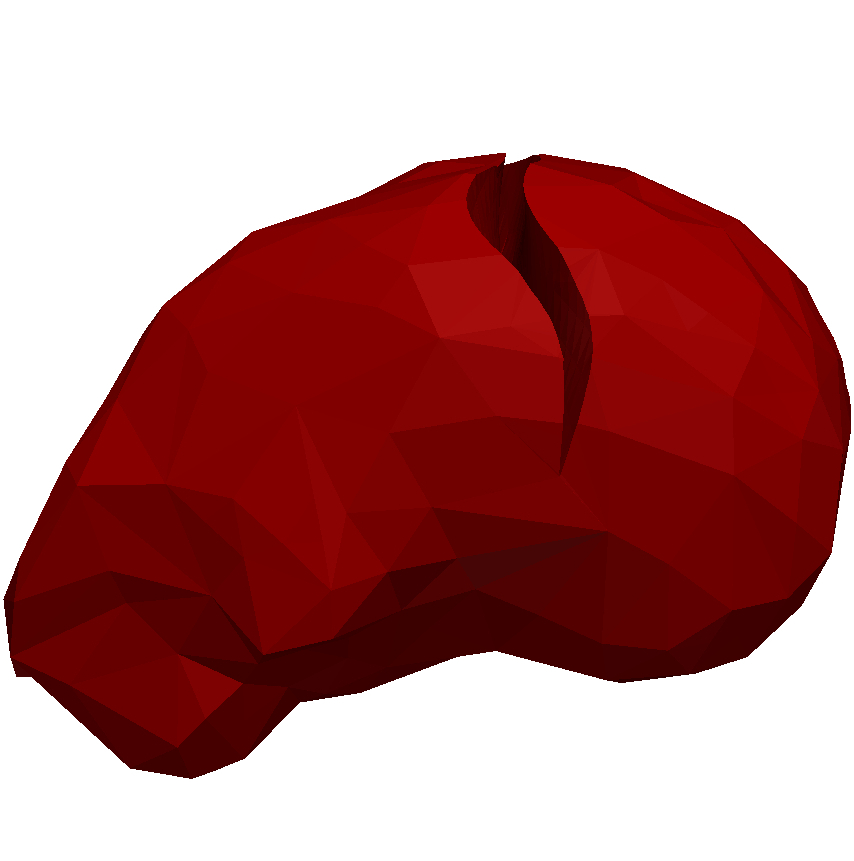
using the extended FEM (X-FEM) that uses shape functions that can model discontinuities inside elements (see Fig. 12 ),
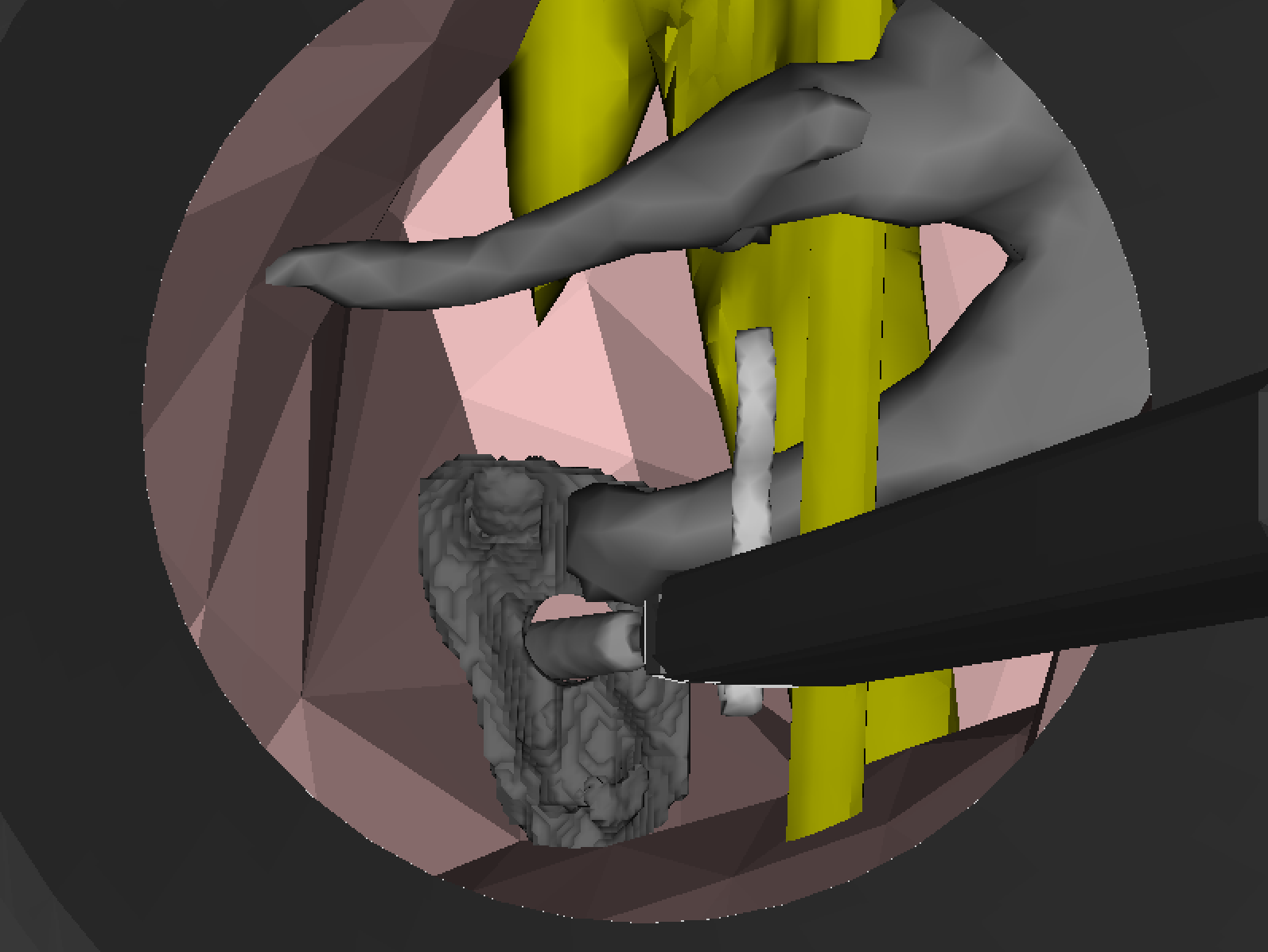
A re-meshing approach to model cuts has been submitted to several conferences, we are waiting for the response. An implementation of the extended finite element method was published in a preprint "Simulation of Complex Cuts in Soft Tissue with the Extended Finite Element Method (X-FEM)". The figures below show a simulation of a sinusoidal cut on a liver executed with the implementation of the X-FEM.
For the LEM approach (see Fig. 11 ), a multimapping between finite elements and lattice model have been developed and implemented into SOFA framework. This allows us to perform a multiscale simulation in real-time. A dynamic changing of topology between finite elements and lattices should be developed in the next step in order to perform the cutting dynamically.
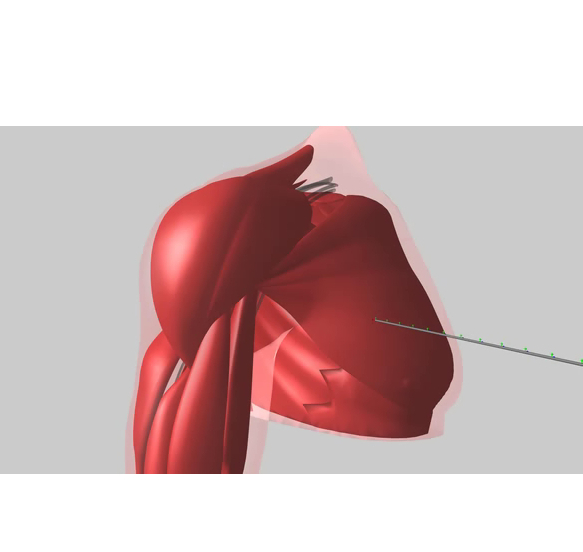
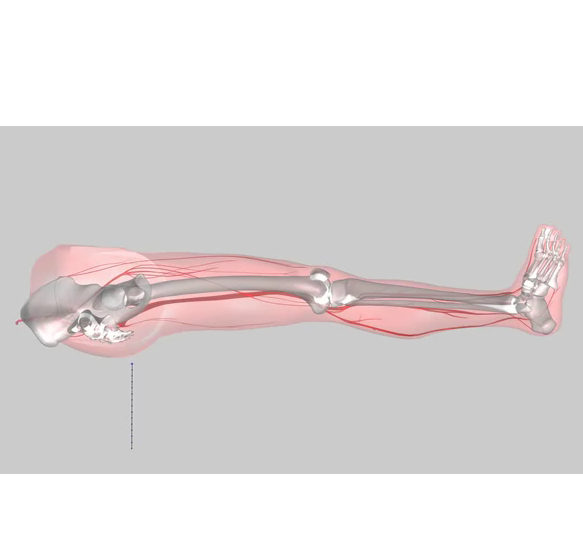
Regional anaesthesia
Participants : Rémi Bessard Duparc, Frédérick Roy.
The RASimAs project (Regional Anaesthesia Simulator and Assistant) is a European research project funded by the European Union's 7th Framework Program. It aims at providing a virtual reality simulator and assistant to doctors performing regional anaesthesia by developing the patient-specific Virtual Physiological Human models. This year, the code for needle insertion has been re-designed and simplified into SOFA and the muscle contraction has been implemented. Finally, the components of the simulation have been optimized to reach the desired real-time performances (i.e more than 25-30 frames per second).
Our preliminary results are awaiting the validation of the Working Packages in January 2015. The needle refactoring will be shared with an other project in Strasbourg (robot) and may be shared with an other team at Inria Rennes with the LAGADIC Team.
|
Control of elastic soft robots
Participant : Frédérick Largillière.
We developed a prototype of stiffness-controlled haptic interface using a piece of silicone rubber to render different forces related to a displacement ie. different stiffnesses and an improved method of simulation using multi-rate loops to try to keep the computation real-time even with models using a large number of FEM elements. (work currently under review) We also presented the idea of a surgical robot able to virtually reconstruct its environment (ie. surrounding biological tissues) through small modifications of the algorithm used for controlling soft robots (SURGETICA 2014).
Image-Driven Simulation
Physics-based registration algorithms
Participant : Rosalie Plantefève.
Before targeting the augmented reality for laparoscopic operations, an important step consists in solving the initial alignment problem. Given a pre-operative image of the organ (usually a CT scan) a detailed mesh is constructed. To make the information stored in this mesh available during the operation, the mesh must be registered onto the intra operative view. However, mainly due to the pneumoperitoneum, the organ has undergone important deformation between the pre-operative images acquisition and the operation. The pre-operative shape and the intra-operative shape of the organ do not correspond. Therefore a non rigid registration is required to align the mesh and the real organ. Our registration algorithms also allowed us to work on a mean to automatically recover boundary conditions of a patient specific liver.
We created a statistical atlas [29] of the human liver to store some of the liver boundary conditions positions : the veina cava and the anchor point of the falciform ligament positions. This method was presented at MICCAI 2014. We also developed a new registration method [28] that evolves automatically from a rigid registration to a non rigid registration to solve the initial alignment problem. The method use some anatomical features of the liver such as the anchor point position of the falciform ligament. This method was presented at ISBMS 2014.
|
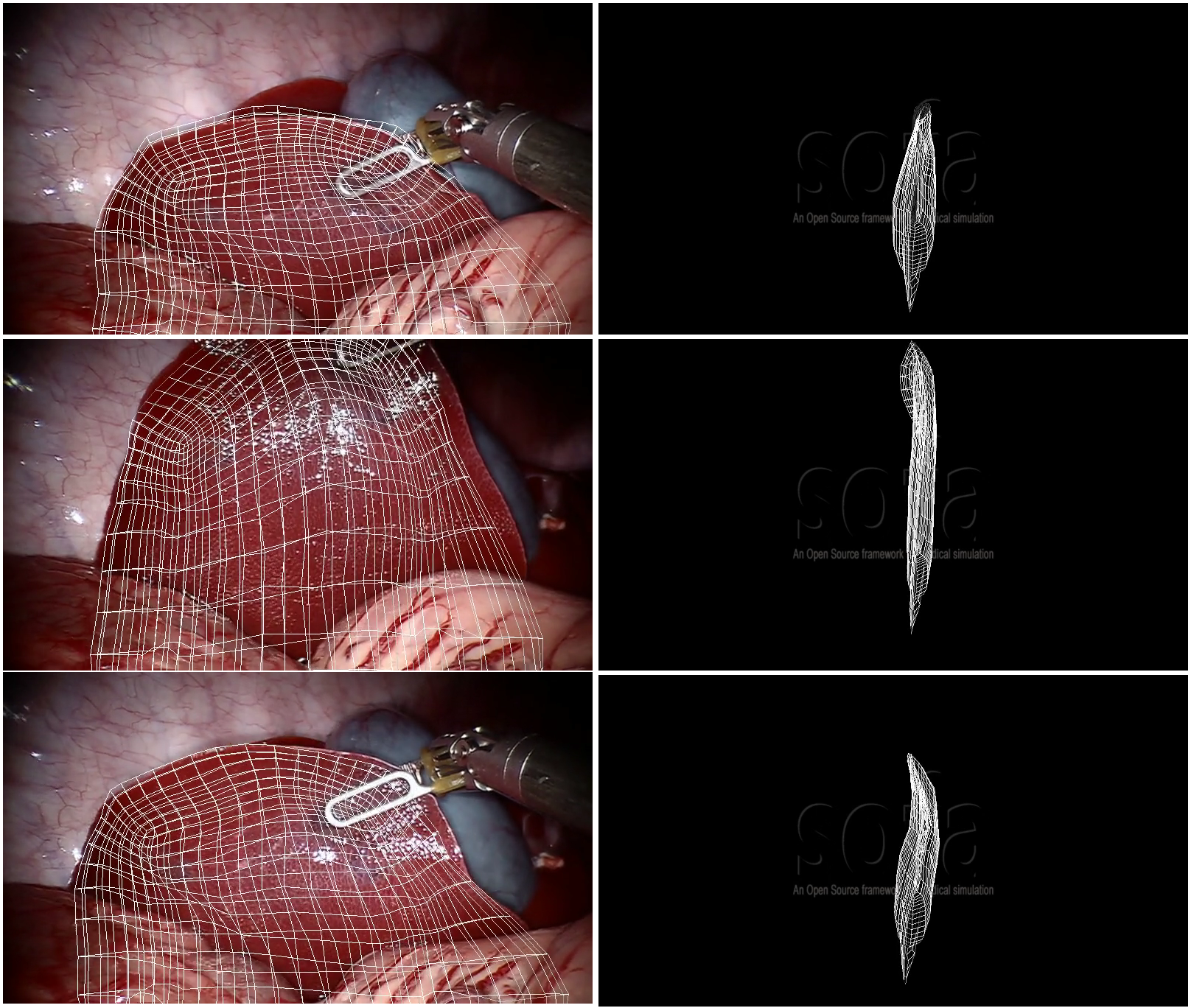
Augmented reality
Participant : Nazim Haouchine.
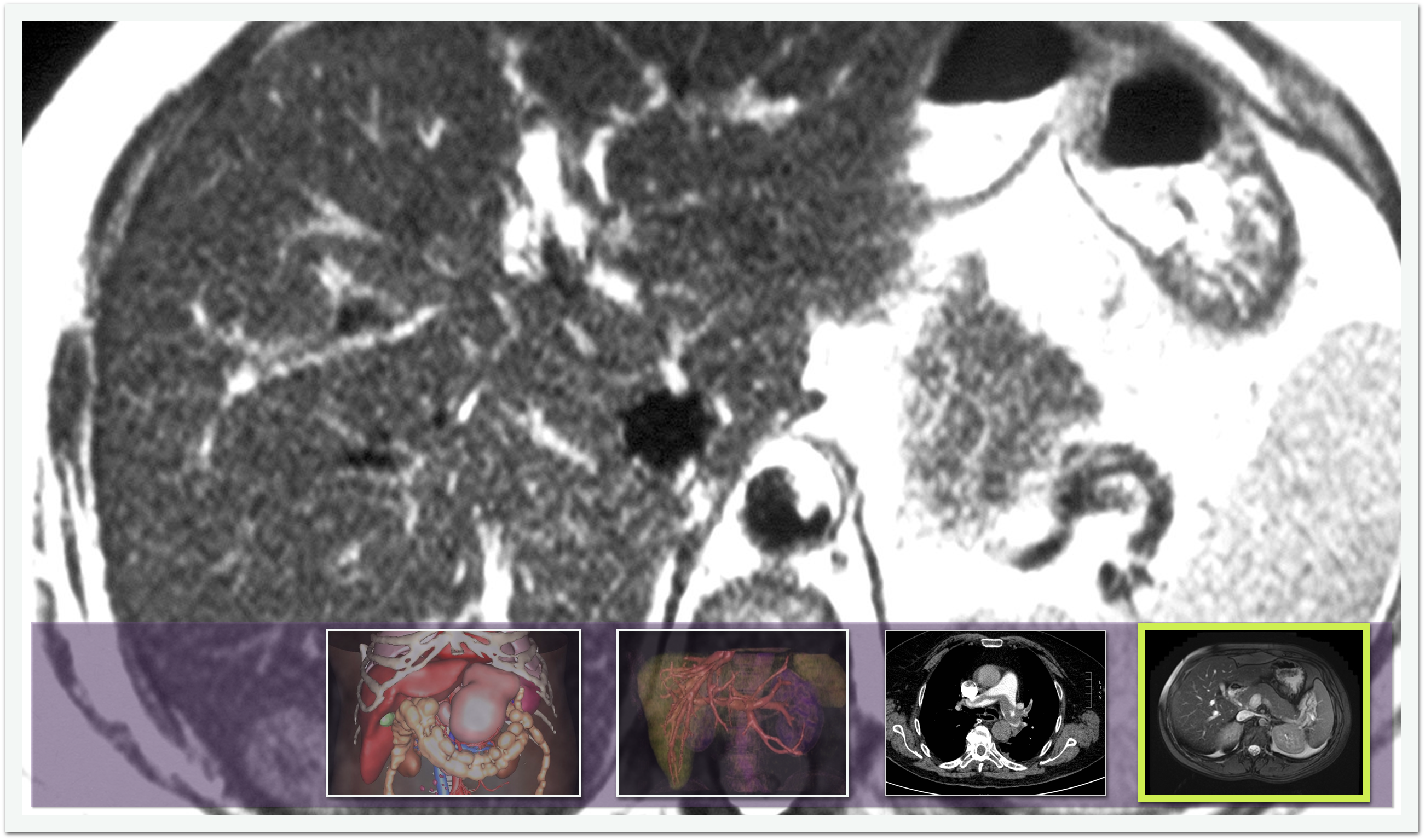
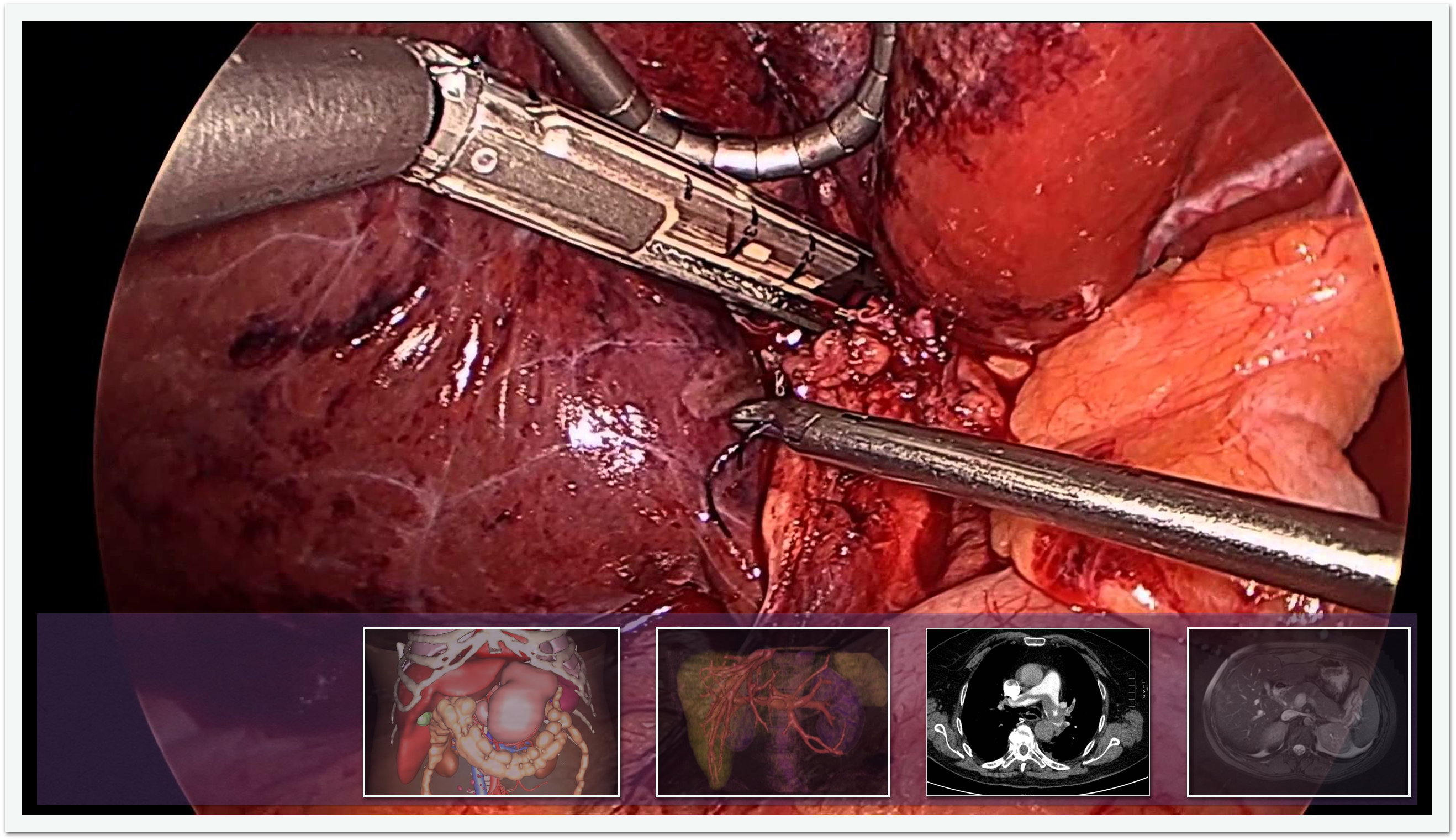
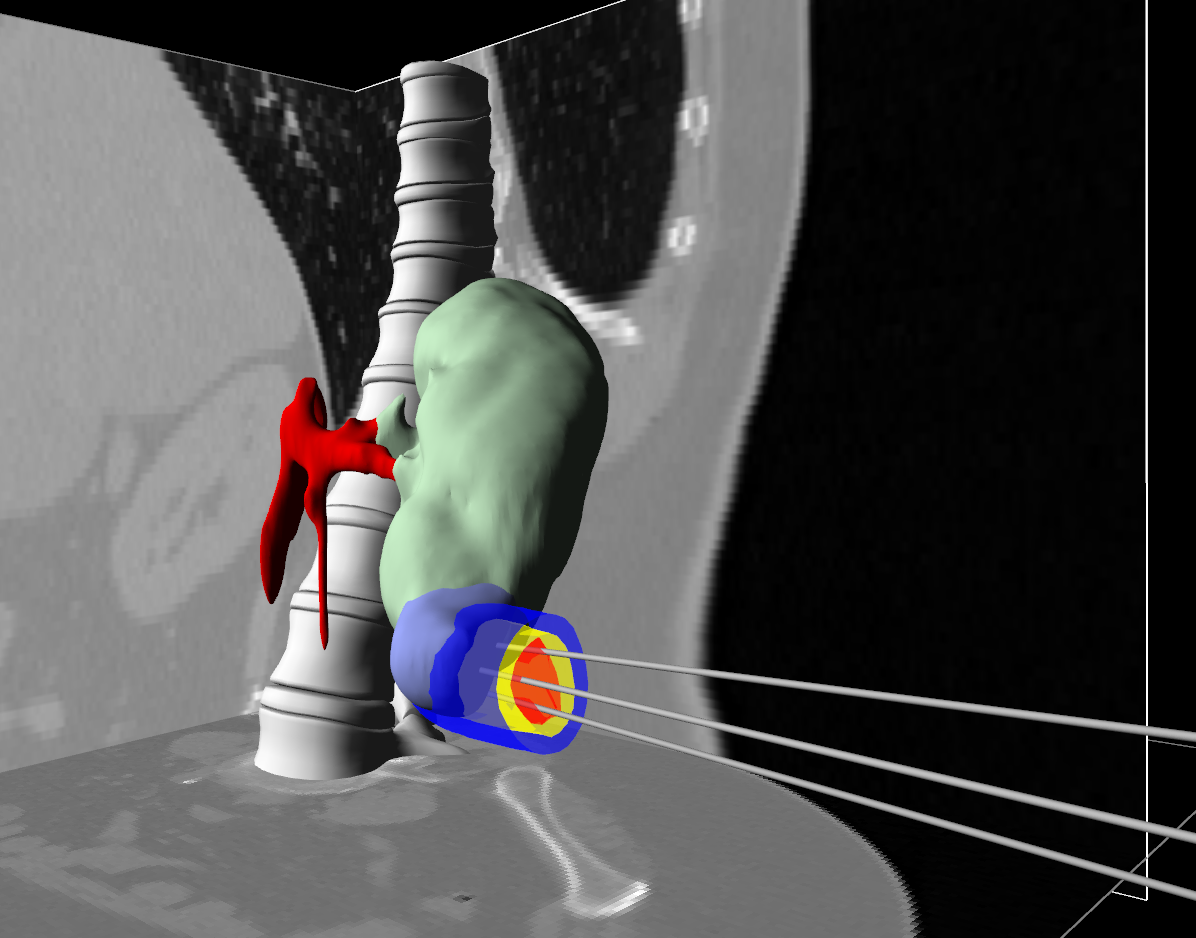
After this intra-operative registration, the augmented reality is possible. This topic is one the highlight of the year 2014. In 2014, we proposed a method for real-time augmented reality of internal liver structures during minimally invasive hepatic surgery [25] . This project is done is collaboration with the EPI MAGRIT. Vessels and tumors computed from pre-operative CT scans can be overlaid onto the laparoscopic view for surgery guidance. Compared to current methods, our method is able to locate the in-depth positions of the tumors based on partial three-dimensional liver tissue motion using a real-time biomechanical model. This model permits to properly handle the motion of internal structures even in the case of anisotropic or heterogeneous tissues, as it is the case for the liver and many anatomical structures. Experimentations conducted on phantom liver permits to measure the accuracy of the augmentation while real-time augmentation on in vivo human liver during real surgery shows the benefits of such an approach for minimally invasive surgery. Finally, a method for 3D reconstruction of elastic shapes with self-occlusion handling was also proposed.
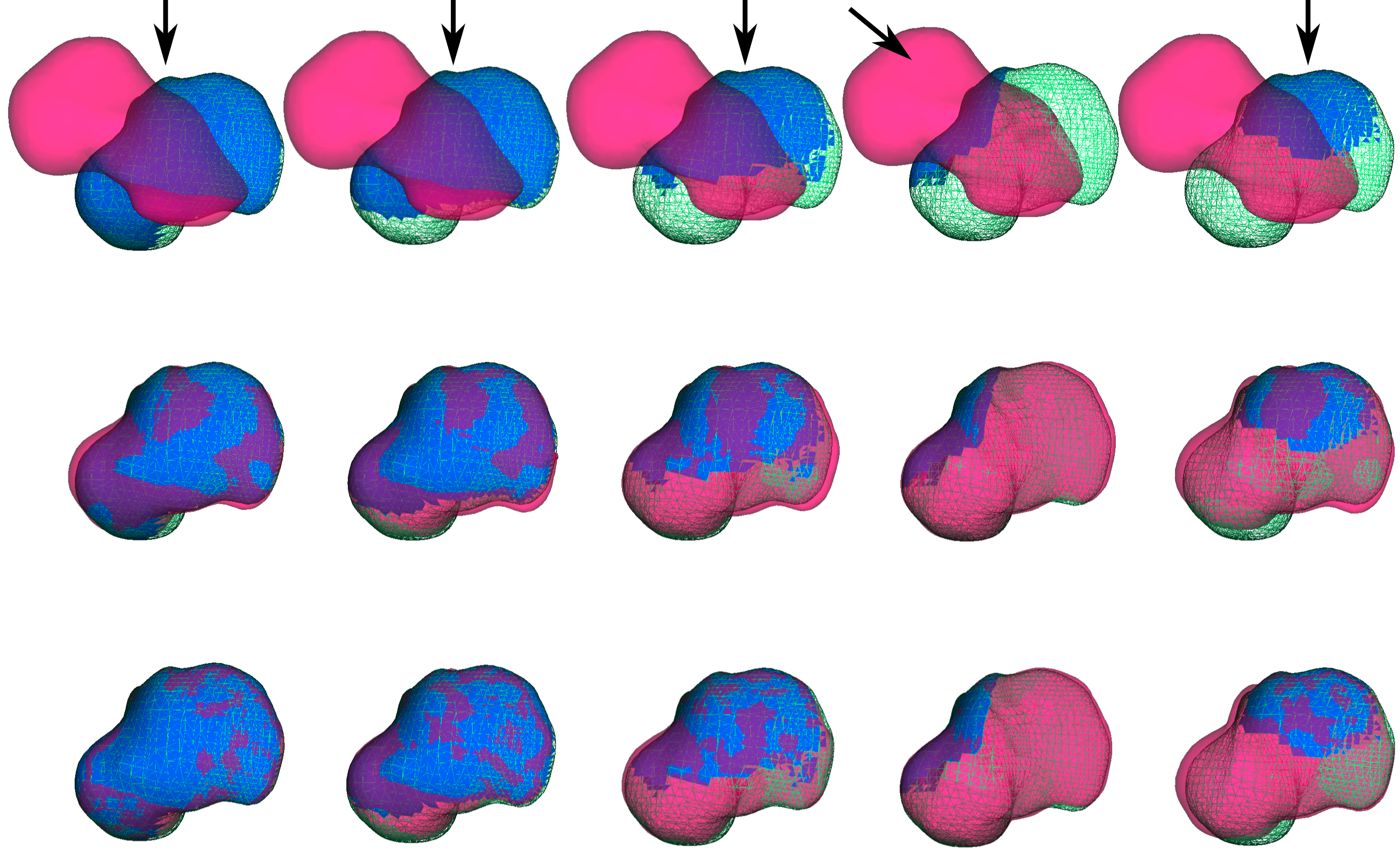
Segmentation
Participant : Zhifan Jiang.
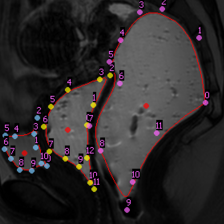
We have been working on medical image analysis in the context of the female pelvic medicine. Image-based diagnoses of pelvic floor disorders like prolapse or endometriosis rely on mechanical indicators, such as mobilities of organs and shear displacements between organs. Image data do not provide directly qualitative indicators hence analysis and diagnosis of medical are required although unfortunately subjected to surgeon expertise subjectivity. Therefore, objective information would be useful for both precise diagnoses and planning of surgical procedure. The objective is to develop numerical tools which extract quantitative information from static and cine MR images based on algorithms of detection and tracking.
We have developed numerical models not only for visualization, but also for quantitative measurements on a group of organs, such as their shapes and their relative movements. The numerical tool extracts these quantitative information (displacements and shear inter-organ) as well as the geometric shape of organs from images via Model-to-Image registration based on B-spline models. Our approach enables to identify multiple organ shapes in a single 2-dimension MR image and then to track their motion in a sequence of 2-dimension dynamic (cine) MR images for the study of the mobilities of the pelvic system. The method has been tested on healthy and pathological patient-specific data (19 patients) and the results provide valuable data to assess the shear displacement between organs and therefore making it possible to identify weakened ligaments or fascia which function differently in patients having pathologies. However, the results are to be validated by further mechanical FEM simulations. This work has been accepted in the journal STRAIN.
MIND project
Participants : Myriam Lekkal, Raffaella Trivisonne.
Within a feasibility study contest, we worked on Human Computer Interaction developing a new, intuitive and efficient way to interact with medical information in modern operating room. Nowadays operating rooms are progressively outfitted with computerized equipment necessary to access and manipulate a significant amount of data (i.e. medical images, patient’s records, patient’s vitals and physical parameters of the operating environment). This type of equipment belongs to the non-sterile section of an operating room, therefore surgeons, who are not allowed to be contaminated, cannot directly interact with it.
The idea of MIND project is to create a new device that could be used alone, such as a remote control, or easily integrated onto several locations, according to user preferences or constraints from the surgical procedure. Through this remote control, surgeons are able to access and manipulate medical information within the operating field and without leaving the instruments. For the software side the main aspects are distributed in two categories: a low level library, in charge of tasks such like handling the communications between the wireless instrument and the central computer, and a set of high-level functionalities and applications concerning the development of users GUI and new applications according to the needs of the case.
This work resulted in a patent [35] (still pending). Read more here http://mindsurgeonmouse.weebly.com/ .